…or, as I called it a few days back, dosage, gets a more technical examination here (the linked article, by the way, is very dense reading, but I urge everyone to plow through it anyway. You may learn something that prevents you from getting infected). A sample:
What evidence do we have that viral load matters?
Three classes of evidence seem strong.
The first is that we have a strong mechanism story we can tell. Viruses take time to multiply. When the immune system detects a virus it responds. If your initial viral load is low your immune system gets a head start, so you do better.
The second category is the terrible outcomes in health care workers on the front lines. Those who are dealing with the crisis first hand are dealing with lots of intense exposures to the virus. When they do catch it, they are experiencing high death rates. High viral load is the only theory I know about so far for why this is the case. Their cases are presumably handled at least as well as others, in terms of detection, testing, treatment and what the infected do themselves. The only other issue I can think of is that they might be reluctant to rest given how urgently their help is needed.
The third category is historical precedents.
Parents infected their children with what they hoped was exactly the minimum dose [of smallpox] required to get them sick enough to develop antibodies and gain immunity. Sometimes this went wrong and the child would get sick. Thus this form of inoculation was dangerous and 1%-2% of patients died. But of those who got smallpox infections in other ways, 20%-30% of patients died. Those rates are well established.
I should point out that Doc Russia, who as an ER doctor has been treating Chinkvirus patients almost daily, fully expected to catch the virus himself, but so far [crossing fingers] hasn’t. All I can think of is that because his hospitals (he works in several) don’t have that many infectees compared to those in, say, London or New York, his aggregate exposure is low; that, his age outside the at-risk group, plus his fanatical adherence to commonsense protective measures, has probably kept him well. Which leads to the other major point in the above linked article:
The default model is that the longer and more closely you interact with an infected person, especially a symptomatic infected person, the larger your viral load.
In-household infections are presumed to be high viral load, as in the case of measles. So would be catching the infection while treating patients.
Most out-of-household infections that aren’t health care related are presumed to be low viral load. Anything outdoors is probably low viral load. Most methods that involve surfaces are probably low viral load. Infection via the air from someone there half an hour ago, to the extent this is a thing, is low viral load. Quick interactions with asymptomatic individuals are probably low viral load.
I should point out that the above are observations based on admittedly-poor data, but as we know that the level of dosage/viral load is critical in other diseases (measles, smallpox, SARS etc.), it’s not a bad deduction to assume that it’s true also of the Chinkvirus.
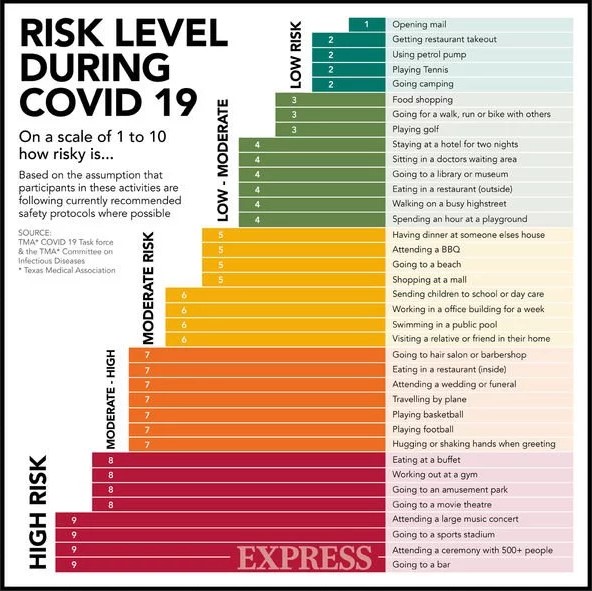
As with all decisions in life, the key to decision-making is risk assessment and odds-calculation. Use all the above accordingly, as you plan your daily life.